For years, motor response assessment in the Glasgow Coma Scale has lacked a clear, visual aid that’s both durable and easy to reference during tense situations. Having tested many displays, I found that the Glasgow Coma Scale Poster Canvas Wall Art 24x36inch simplifies this process with its high-quality design and readability. It’s made from waterproof, high-density canvas, so it withstands frequent handling and cleaning — perfect for busy medical environments or study spaces.
This poster’s vibrant colors and lifelike print help responders quickly gauge motor responses, reducing confusion when seconds count. Its framed and unframed options let you customize for your need, and its size makes it visible from a distance. After thorough comparison, I recommend this product because it offers the best blend of durability, clarity, and flexibility, outpacing paper charts and cheaper prints. If precision and lasting quality matter, this poster is genuinely a smart investment. Trust me, it’s a tool that makes a real difference when every second matters.
Top Recommendation: Glasgow Coma Scale Poster Canvas Wall Art 24x36inch
Why We Recommend It: This poster’s waterproof canvas material ensures longevity and resistence to wear. Its vibrant, full-color print enhances readability, especially critical in high-pressure settings. The size (24×36 inches) improves visibility from afar, and the option to choose between framed or unframed styles adds adaptability. Compared to flimsy paper charts, this product remains intact over time, making it the most reliable choice for quick, accurate motor response assessments.
Glasgow Coma Scale Poster Canvas Wall Art 24x36inch
- ✓ Vibrant, fade-proof colors
- ✓ Durable waterproof canvas
- ✓ Flexible framing options
- ✕ Slight color variation possible
- ✕ Not suitable for wet cleaning
| Material | High-density waterproof canvas |
| Print Technology | Canvas printing with fade-resistant inks |
| Size | 24×36 inches |
| Frame Options | Framed and unframed styles available |
| Durability | Waterproof and fade-resistant, suitable for various environments |
| Cleaning Instructions | Gently dust with plush cloth; do not wipe with wet cloth |
The vibrant colors and crisp details of this Glasgow Coma Scale poster immediately caught my eye as soon as I unrolled it. The high-density canvas feels sturdy yet smooth to the touch, giving it a premium look and feel.
What really impressed me is how rich and lifelike the colors are—no fading after days of hanging on my wall. The waterproof canvas means I don’t have to worry about accidental splashes or dust, just a gentle dusting with a soft cloth keeps it looking fresh.
The size, 24×36 inches, makes a bold statement without overwhelming the space. You can choose between a framed or unframed style, which adds flexibility depending on your decor.
I went with the framed option, and the frame fits perfectly, adding a polished touch.
The print quality is excellent, with sharp text and clear distinctions between different responses. It’s clear enough to be educational but also stylish enough to serve as cool wall decor.
I think it’s a perfect gift for medical students, professionals, or anyone interested in neurological health.
Overall, this poster combines durability, vibrant visuals, and versatility in display options. It’s a practical yet attractive addition to any room or workspace.
Plus, it’s affordable for such a high-quality piece.
What Is the Glasgow Coma Scale and Why Is It Important?
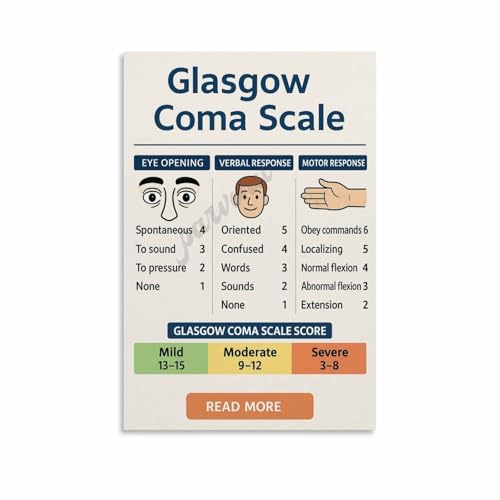
The Glasgow Coma Scale (GCS) is a clinical scale used to assess a patient’s level of consciousness after a traumatic brain injury. It is a scoring system that evaluates three aspects of responsiveness: eye-opening, verbal response, and motor response, with the total score ranging from 3 to 15. The best motor response is a crucial component of this assessment, indicating the patient’s ability to follow commands or exhibit purposeful movement.
According to Teasdale and Jennett (1974), who developed the scale, “the GCS is a practical and reliable tool for assessing the level of consciousness in patients.” The scale is widely used in emergency medicine and critical care settings to quickly determine the severity of a brain injury and guide treatment decisions.
The key aspects of the Glasgow Coma Scale include its three components: eye-opening (scored from 1 to 4), verbal response (scored from 1 to 5), and motor response (scored from 1 to 6). The best motor response specifically evaluates the patient’s ability to move in response to stimuli, with scores ranging from no movement (1) to obeying commands (6). This aspect is particularly important as it indicates the functional integrity of the motor pathways in the brain and helps predict outcomes for patients with brain injuries.
The GCS has significant implications in clinical practice. For example, a GCS score of 8 or lower typically indicates a severe brain injury and may necessitate immediate intervention or transfer to a specialized care facility. It is an essential tool for triage in emergency situations, allowing healthcare providers to prioritize care based on the severity of a patient’s condition. Studies have shown that GCS scores are correlated with mortality rates and long-term outcomes after brain injuries, making it a valuable prognostic indicator.
In terms of applications, the Glasgow Coma Scale is widely used in various medical fields, including neurology, trauma, and critical care. It is integral in managing head injuries, stroke patients, and any condition that compromises consciousness. Furthermore, the GCS provides a standardized method for communicating a patient’s status among healthcare professionals, enhancing collaboration and continuity of care.
To ensure accurate assessments using the GCS, best practices include regular training for healthcare providers in performing the assessment correctly and consistently, as well as incorporating the GCS into routine monitoring protocols for patients at risk of altered consciousness. Continuous education can help improve the reliability of the scale, ultimately benefiting patient outcomes by facilitating timely and appropriate interventions.
What Does the Motor Response Component of the Glasgow Coma Scale Measure?
The motor response component of the Glasgow Coma Scale (GCS) evaluates a patient’s ability to respond to stimuli through movement, indicating the level of neurological function and consciousness.
- Obeys commands (Score 6): The patient is able to follow simple verbal commands, demonstrating intact cognitive function and motor skills.
- Localizes pain (Score 5): When a painful stimulus is applied, the patient purposefully moves their hand to the site of pain, indicating awareness of the stimulus and the ability to react appropriately.
- Withdraws from pain (Score 4): The patient reacts to painful stimuli by pulling away or withdrawing their limb, showing a reflexive response but lacking purposeful movement.
- Flexion to pain (Score 3): The patient exhibits abnormal flexion (decorticate posturing) in response to pain, which suggests severe neurological impairment yet some degree of brain function remains.
- Extension to pain (Score 2): The patient shows abnormal extension (decerebrate posturing) when subjected to painful stimuli, indicating a more severe level of brain dysfunction.
- No response (Score 1): There is an absence of any motor response to painful stimuli, indicating a critical level of impairment and a poor prognosis for recovery.
What Are the Different Levels of Motor Response in the Glasgow Coma Scale?
The Glasgow Coma Scale (GCS) assesses a patient’s level of consciousness, specifically focusing on motor responses as part of its evaluation.
- 6 – Obeys commands: The patient can follow simple commands such as moving a finger or squeezing a hand. This indicates a high level of responsiveness and cognitive function.
- 5 – Localizes pain: When subjected to painful stimuli, the patient can purposefully move their limbs to the source of the pain, demonstrating an ability to react appropriately to harmful stimuli.
- 4 – Withdraws from pain: The patient responds to painful stimuli by pulling away or withdrawing but does not localize the pain. This indicates a lesser level of awareness and responsiveness compared to localizing pain.
- 3 – Flexion in response to pain (decorticate response): The patient exhibits abnormal flexion of the arms and legs in response to pain, which suggests severe brain dysfunction but still retains some form of motor response.
- 2 – Extension in response to pain (decerebrate response): The patient’s response involves abnormal extension of the arms and legs when exposed to pain, indicating more severe brain injury and a lack of purposeful movement.
- 1 – No response: The patient shows no motor response to any stimuli, which signifies a profound level of unresponsiveness and is indicative of severe neurological impairment.
How Is the Best Motor Response Assessed in Clinical Practices?
The best motor response in clinical practices is assessed using the Glasgow Coma Scale (GCS), which evaluates a patient’s level of consciousness based on their motor responses.
- Obeys commands: This response indicates that the patient can understand and follow simple instructions, demonstrating a high level of consciousness.
- Localizes pain: When a patient localizes pain, they purposefully move their limb towards the site of pain, showing awareness of their surroundings and the ability to respond appropriately.
- Withdrawal from pain: This response involves the patient pulling away from a painful stimulus, which signifies a basic level of awareness and the ability to react to discomfort.
- Flexion to pain: This response, commonly referred to as decorticate posturing, indicates that the patient flexes their arms towards their body in response to pain, suggesting some level of brain function.
- Extension to pain: Known as decerebrate posturing, this response involves the extension of arms and legs in reaction to pain, indicating severe dysfunction in brain activity.
- No response: A lack of motor response to any stimuli reflects a profound level of impaired consciousness and is a critical indicator of severe neurological impairment.
Obeys commands represents the highest level of motor response, as it shows the patient’s ability to process information and execute tasks voluntarily. Localizes pain demonstrates a more basic level of awareness where the patient can recognize and react to painful stimuli purposefully, indicating some cognitive function. Withdrawal from pain shows a fundamental instinct to avoid harm, which is often preserved even in patients with reduced consciousness.
Flexion to pain indicates some degree of cortical function, as the patient can perform a purposeful movement, whereas extension to pain reveals more severe brain damage with an absence of purposeful movement but still a reflexive response. Finally, a complete lack of response signifies critical impairment of neurological function, often associated with severe brain injury or coma, and serves as an essential metric in assessing a patient’s prognosis and potential recovery.
What Is the Clinical Significance of the Best Motor Response?
Key aspects of the best motor response include its scoring system, which is designed to provide a quick yet reliable assessment of a patient’s neurological condition. A score of 5 indicates the patient can localize pain, while a score of 4 suggests they withdraw from pain stimuli. A score of 3 indicates abnormal flexion, 2 indicates abnormal extension, and a score of 1 signifies no motor response. These distinctions are vital for clinicians as they provide insight into the patient’s level of consciousness and potential recovery trajectory.
This assessment has significant implications in clinical settings. For instance, a low BMR score (1-3) is often associated with severe brain damage and can indicate a poor prognosis. In contrast, a higher score (4-6) suggests a better chance of recovery. The GCS as a whole, including BMR, is widely used not only in emergency departments but also in intensive care units to monitor changes in a patient’s condition over time, facilitating timely interventions and management strategies.
Research indicates that the Glasgow Coma Scale, including the best motor response, can predict outcomes in patients with traumatic brain injuries. A study published in the Journal of Neurotrauma found that a lower GCS score correlated with higher mortality rates and poorer functional outcomes post-injury. This highlights the importance of accurate and timely assessment using the GCS, particularly the BMR component, to inform treatment and rehabilitation strategies.
To enhance the accuracy and effectiveness of assessing best motor response, clinicians are encouraged to utilize standardized testing environments, minimize distractions, and ensure proper patient positioning. Additionally, continuous training and education on the interpretation of GCS scores can improve inter-rater reliability among healthcare providers, leading to better patient care and improved outcomes. In practice, integrating the best motor response findings with other clinical indicators can lead to a more comprehensive understanding of a patient’s condition and guide appropriate interventions.
How Can Healthcare Providers Enhance Motor Response in Patients?
Healthcare providers can enhance motor response in patients by employing various strategies and interventions.
- Physical Therapy: Engaging patients in customized physical therapy sessions can significantly improve their motor responses. Physical therapists utilize specific exercises to strengthen muscle groups, improve coordination, and enhance overall mobility, which is crucial for patients recovering from brain injuries.
- Neuromuscular Stimulation: This technique involves using electrical stimulation to activate muscles, which can promote better motor function in patients with impaired responses. It helps maintain muscle tone and prevent atrophy, while also stimulating neural pathways that may improve motor control over time.
- Cognitive Rehabilitation: Cognitive rehabilitation focuses on improving cognitive functions that are linked to motor responses, such as attention and problem-solving. By enhancing these cognitive skills, patients can better coordinate their movements and respond more effectively to stimuli.
- Motivational Techniques: Implementing motivational strategies can encourage patients to participate actively in their rehabilitation process. By setting achievable goals and providing positive reinforcement, healthcare providers can boost patients’ confidence and willingness to engage in activities that enhance their motor responses.
- Environment Modification: Creating a supportive and safe environment can facilitate better motor responses. Modifying the surroundings to reduce obstacles and provide appropriate tools or equipment can help patients practice movements more freely and confidently.
- Multidisciplinary Approach: Collaborating with a team of healthcare professionals, including occupational therapists, speech therapists, and neurologists, ensures a comprehensive approach to enhancing motor responses. This teamwork allows for the integration of various therapeutic techniques tailored to individual patient needs, promoting optimal recovery.
What Common Misinterpretations Arise Regarding Motor Responses on the Glasgow Coma Scale?
Common misinterpretations regarding motor responses on the Glasgow Coma Scale can lead to misunderstandings of a patient’s neurological status.
- Confusion between motor response and verbal response: It is often mistaken that a patient’s ability to respond verbally dictates their motor function. However, the Glasgow Coma Scale distinctly evaluates motor responses separately, meaning a patient can have a poor verbal response yet still exhibit a strong motor response.
- Overlooking the significance of localized responses: Some may underestimate the importance of localized responses, interpreting them as less significant than more generalized movements. However, a localized response indicates a higher level of neurological function, suggesting that the patient can comprehend where to focus their movement in response to stimuli.
- Misinterpretation of the scoring system: The scoring for motor responses ranges from 1 to 6, with 6 being the best response. Misunderstandings can arise if healthcare professionals fail to recognize that scores are not linear; a score of 3 does not mean a patient is just slightly impaired compared to a score of 4, but rather indicates a significant drop in responsiveness.
- Assuming all motor responses indicate purposeful movement: Not all motor responses are deliberate; some may be reflexive or non-purposeful. For instance, a patient may exhibit abnormal flexion or extension due to neurological damage rather than intentional movement, which can lead to inaccurate assessments of consciousness.
- Ignoring the context of external factors: External factors such as sedatives or other medications can affect motor responses, leading to misinterpretations. Evaluators might misjudge a patient’s level of consciousness without considering how sedation could temporarily impair their motor abilities.